Hernia after Iliac Crest Bone Grafting- Case Report of A Rare Complication
Vol 1 | Issue 1 | Jan-Apr 2016 | page:14-16 | Chirag Borana[1], Lokesh Sharoff[1*], Naeem Jagani[1], Nadir Shah[1], Chitrangada Singh[2].
Author: Chirag Borana[1], Lokesh Sharoff[1*], Naeem Jagani[1], Nadir Shah[1], Chitrangada Singh[2].
[1] Grant Government Medical College and Sir J.J group of Hospitals, Mumbai.
[2] D.Y.Patil Medical College and Research Centre, Nerul, Navi Mumbai.
Address of Correspondence
Dr. Lokesh Sharoff
42, Madhur Milan Society, 14 th B road, Khar west, Mumbai – 400052
Email : drlokeshsharoff@outlook.com
Abstract
Background: The most common site of bone grafting is from the iliac crest. It can provide cancellous, cortical as well as cortico-cancellous grafts and also is an abundant source of bone graft. It is associated with various complications. Hernia through the iliac crest bone grafting is a very rare complication. This complication can be prevented if necessary steps are taken during surgery and hence we describe this case report to help prevent this complication which usually requires another surgery.
Keywords: Hernia, Bone-Grafts, Complication, Swelling, Case-Report.
Introduction
Bone grafting is a frequently performed procedure in Orthopaedic surgery. Usually it is performed for non-unions or comminuted fractures. Autologous bone graft provides osteoconduction, osteoinduction and osteogenesis effect. The most common site of bone grafting is from the iliac crest. It can provide cancellous, cortical as well as cortico-cancellous grafts and also is an abundant source of bone graft[1]. It is associated with various complications but hernia through the iliac crest bone grafting site is a rare and major complication which we describe in our case.
Case Presentation
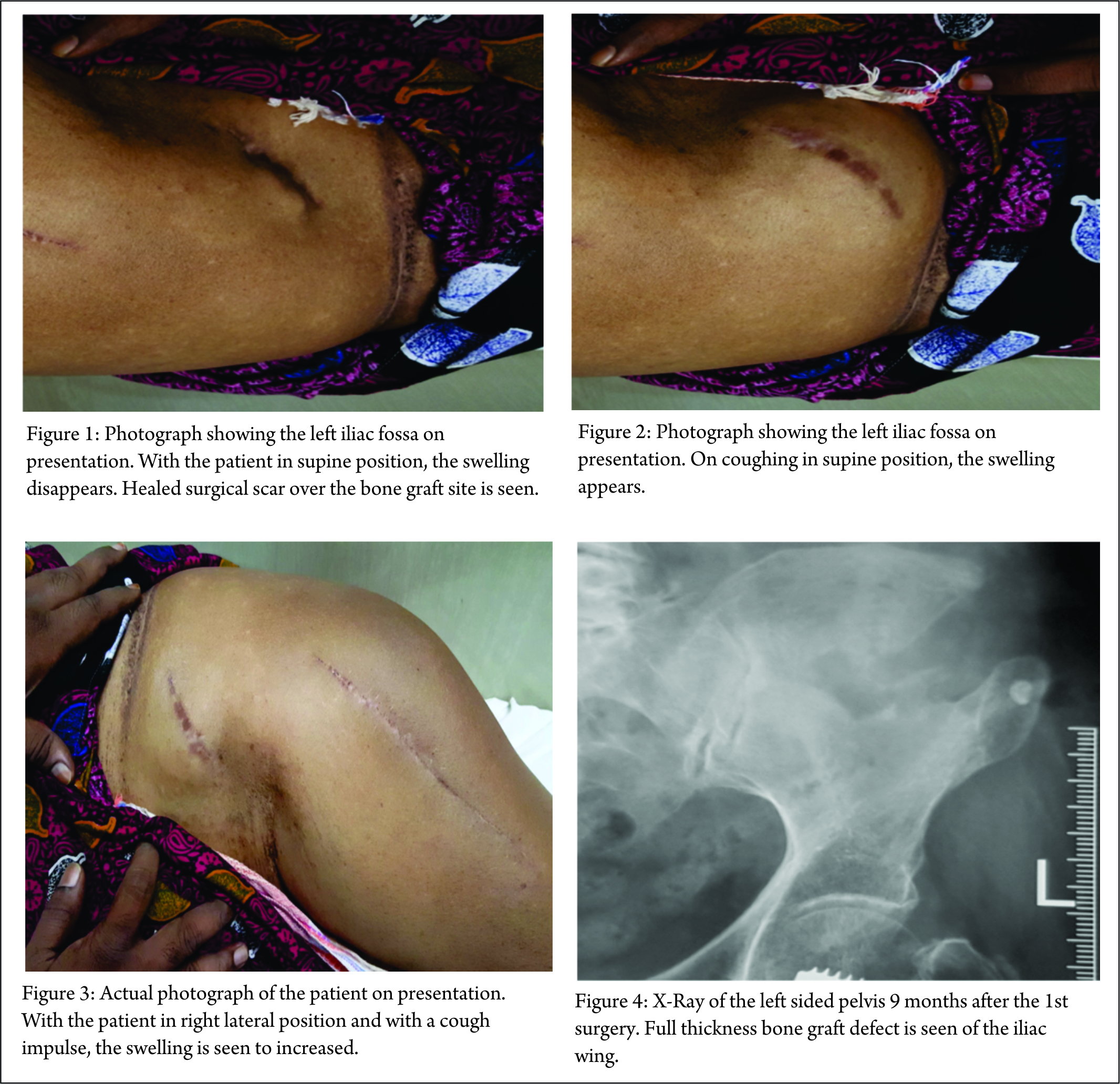
80 years old lady came to the orthopaedic OPD with complaints of swelling over the left flank since 1 month [Fig. 1] which was more prominent on coughing [Figure 2,3] and raising the intra-abdominal pressure during defecation. She also had abdominal pain. 10 months back, she suffered a left subtrochanteric femur fracture for which DHS and primary bone grafting (from the left iliac crest) was performed due to osteoporotic bone. Clinically, she had a soft reducible swelling over the incision site, which increased during coughing and standing and reduced while lying down. Swelling was non-pulsatile and no other swelling was present anywhere else in the body. Xray at presentation showed a large, full thickness defect of the left iliac crest bone grafting site[Fig. 4]. Patient was advised repair but was not ready for another surgery. She has been advised regular follow up and is informed about complications like incarceration or strangulation that can arise due to hernia.
Discussion
There are reported complications related to the donation of autogenous bone from the iliac crest. Our review revealed reports of arterial injury, ureteral injury, herniation, chronic pain, nerve injury, infection, fracture, pelvic instability, cosmetic defects, hematoma[1]. The occurrence of hernia through iliac crest bone defect was first reported by Oldfield in 1945[2].The current incidence is unknown. In a series of 59 iliac grafts, the incidence of this complication was 5%. It is more common in females[3].The onset of symptoms ranges from 24 days to15 years postoperatively[4]. The first symptom is the development of a soft tissue mass over the graft site with varying degrees of abdominal discomfort. Colicky abdominal pain and abdominal distension may also be present. Occasionally, patients may present acutely with intestinal obstruction or strangulation (16%)[5]. Plain radiographs will show the bony defect in the ilium and frequently loops outside the wing of ilium will be evident[5]. Computed tomography (CT) is commonly used to confirm the diagnosis, as it helps to delineate the defect in the iliac crest, shows the contents of the sac, and helps to define the fascial planes that may be distorted by the previous surgery[5]. A variety of procedures have been used to obliterate the defect in the iliac crest. These include transfer of anterior superior iliac spine inferiorly and posteriorly with muscle and fascia, use of gluteal fascia and lumbar fascia[6]. The most commonly used method is reinforcement by synthetic mesh[6]. Avoiding full-thickness graft harvesting, preservation of the inner table of iliac crest and secure reattachment of fascial layers and tendons is recommended to avoid development of hernia through the iliac crest defect[6]. Full thickness graft from middle of the iliac crest should be avoided as reattachment of periosteum and fascia is difficult. In an obese patient with poor musculature and a large, full thickness defect (more than 4 cm2), use of polypropelene mesh during primary surgery is advocated [6]. In few special cases like spine surgery that are done through transthoracic approach offer additional advantage. Here the graft defect can be reconstructed using ribs that were removed during exposure [8]. In view of further complications a repair is always advisable [9] and in case patient refuses, an informed consent from the patient regarding understanding the further complications and refusal for treatment should be obtained.
Conclusion
We have reported a very rare complication. Care should be taken in all surgeries of iliac crest bone grafting to avoid this complication. This complication has its own set of complications and requires a repeat surgery most of the time.
Clinical Message
Hernia through iliac crest bone graft site is rare but real complications. Risk factors like obesity, size of graft, reconstruction of fascia and soft tissue should be kept in mind while harvesting the graft. Treatment in form of mesh repair should be advocated to prevent further complications.
References
1. Seiler JG 3rd, Johnson J. Iliac crest autogenous bone grafting: donor site complications. J South Orthop Assoc.2000 Summer;9(2):91-7. PMID:10901646.
2. Oldfield MD. Iliac hernia after bone grafting. Lancet 1945; 248:810-2.
3. Auleda J, Bianchi A, Tibau R, et al: Hernia through iliac crest defects. IntOrthop.1995;19:367-9.
4. Cowley PS, Anderson LD: Hernias through donor sites for the iliac bone grafts. J Bone Joint Surg Am. 1983;65:1023-5.
5. Velchuru Vamsi, Satish Sandesh, Petri John, Sturzaker Hugh. Hernia through an Iliac Crest Bone Graft Site-Report of a Case and Review of the Literature. Bulletin of the Hospital for Joint Diseases.2006; Volume 63, Numbers 3 & 4.
6. Pande Ketan, Pande Sonali, Tomey Sudhir. Hernia through iliac crest defect post bone graft harvesting: a rare complication. Brunei Int Med J. 2013; 9 (2): 114-117.
8. Dave B, Modi H, Gupta A, Nanda A. Reconstruction of iliac crest with rib to prevent donor site complications: A prospective study of 26 cases. Indian J Orthop. 2007 Jul;41(3):180-2.
9. d’Hondt S, Soysal S, Kirchhoff P, Oertli D, Heizmann O. Small bowel obstruction caused by an incarcerated hernia after iliac crest bone harvest. ISRN Surg. 2011;2011:836568.
| How to Cite this article: Borana C, Sharoff L, Jagani N, Shah N, Singh C. Hernia after Iliac Crest Bone Grafting- Case Report of A Rare Complication. Journal of Orthopaedic Complications Jan-April 2016; 1(1):14-16. |