Intraoperative Guide Wire Breakage during Intertrochanteric Fracture Fixation: A Technical Complication and Management Strategy
Vol 2 | Issue 2 | May-August 2025 | page: 8-10| Sachin Kale, Arvind Vatkar, Sushant Srivastava, Abhishek Bhati, Aditya Vyas, Ashok Shyam
Submitted Date: 11-2-2025, Review Date: 09-03-2025, Accepted Date: 12-05-2025 & Published Date: 10-07-2025
https://doi.org/10.13107/joc.2025.v02.i02.22
Authors: Sachin Kale [1], Arvind Vatkar [2], Sushant Srivastava [1], Abhishek Bhati [1], Aditya Vyas [1], Ashok Shyam [3]
[1] Department of Orthopaedics, D.Y Patil School of Medicine and Hospital, Navi Mumbai, Maharashtra, India.
[2] Department of Orthopaedics, MGM Medical College, Navi Mumbai, Maharashtra, India.
[3] Department of Orthopaedics, Sancheti Institute for Orthopaedics and Rehabilitation, Pune, Maharashtra, India
Address of Correspondence
Dr. Sachin Kale,
Department of Orthopaedics, D.Y Patil School of Medicine and Hospital, Navi Mumbai, Maharashtra, India.
E-mail: sachinkale@gmail.com
Abstract
Introduction: Intertrochanteric femur fractures are common orthopaedic injuries in the elderly. Internal fixation using cephalomedullary nails is the standard of care. While generally safe, intraoperative technical complications such as guide wire breakage can pose significant challenges.
Case Report: We report a case of intraoperative guide wire breakage during reaming for cephalomedullary nailing in a 65-year-old female with an intertrochanteric femur fracture. The broken guide was embedded within the femoral neck and managed intraoperatively.
Discussion: Guide wire breakage is a rare but important complication. Causes include equipment fatigue, excessive force, improper technique, and repeated usage. Prevention strategies, intraoperative retrieval techniques, and decision-making protocols are discussed.
Conclusion: Understanding the causes and management of intraoperative guide wire breakage is essential for all orthopedic surgeons. Early recognition, preparedness, and communication are key to optimal patient outcomes.
Keywords: Intertrochanteric fracture, Guide wire breakage, Intraoperative complication, Cephalomedullary nail, Orthopaedic surgery
Introduction
Intertrochanteric fractures account for approximately 45% of all hip fractures and are increasingly prevalent due to the aging population [1]. Cephalomedullary nailing is widely accepted as the standard surgical treatment, offering biomechanical advantages and early mobilization [2]. However, intraoperative technical complications may occur, one of which is guide wire breakage during the reaming process.
Though rare, this complication can disrupt the surgical flow, risk neurovascular injury, and compromise fixation quality. Proper preoperative planning, technique, and handling of instruments are critical in mitigating such risks.
Case Report:
A 65-year-old female presented with a right-sided intertrochanteric femur fracture following a ground-level fall. Standard imaging confirmed an AO/OTA 31-A2 fracture pattern. Under spinal anesthesia and using a traction table, the fracture was reduced and stabilized.
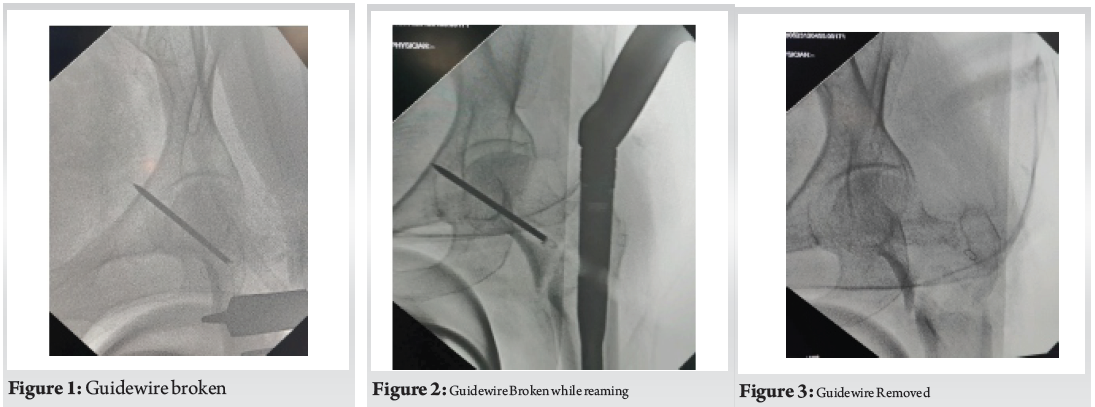
During cephalomedullary nailing, while reaming over the guide wire for the proximal lag screw, resistance was encountered followed by sudden loss of resistance. Fluoroscopic imaging revealed a broken guide wire lodged in the femoral neck (Fig. 1, 2). Attempts at removal with a pituitary rongeur were unsuccessful. (Fig. 3)
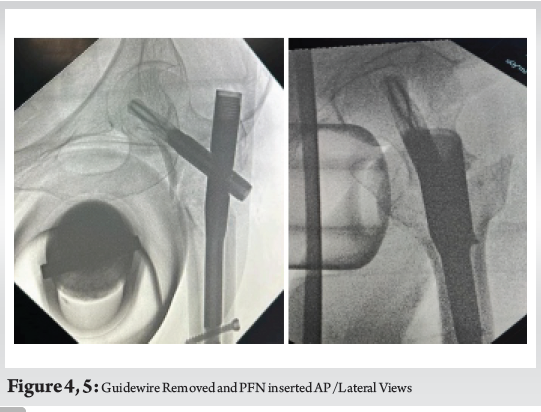
The surgical team proceeded with careful re-reaming through a new trajectory and completed the procedure using a slightly altered entry point and Proximal Femoral Nail was inserted (Fig. 4, Fig. 5). The patient was informed postoperatively, and serial radiographs showed no migration. She progressed to full weight-bearing by 10 weeks.
Discussion:
Causes of Guide Wire Breakage
• Material Fatigue: Repeated use of guide wires beyond recommended cycles leads to metal fatigue [3].
• Forceful Reaming: Excessive resistance during reaming, especially in sclerotic bone, may transmit shearing stress to the wire.
• Improper Trajectory: Misalignment increases the chance of binding and stress concentration.
• Reuse of Instruments: Repeated autoclaving and sterilization can degrade metallic integrity [4].
Prevention
• Use new or certified guide wires whenever possible.
• Avoid forceful advancement of reamers; instead, allow the tool to follow the canal trajectory.
• Always monitor alignment under fluoroscopy.
• Inspect guide wires preoperatively for bending, discoloration, or wear.
Management Options
• Immediate Removal: If accessible, use a pituitary rongeur or cannulated extractor [5].
• Trephine Extraction: Specialized hollow reamers can core around the wire for removal.
• Leave In Situ: If deeply embedded and asymptomatic, retaining the wire may be acceptable with informed consent and documentation [6].
Reporting and Counseling
• Transparency with patients and relatives regarding intraoperative events is essential.
• Proper documentation in operative notes helps in legal protection and academic auditing.
• Reporting such complications improves collective learning, surgical protocols, and patient outcomes [7].
Conclusion:
Guide wire breakage during intertrochanteric fracture fixation is an avoidable but significant complication. Understanding causative factors, employing preventive strategies, and having a clear intraoperative management plan are critical. Surgeons must also prioritize transparent patient counseling and reporting to ensure ethical standards and improve surgical safety.
Clinical Message: Orthopaedic surgeons should be vigilant for potential technical failures such as guide wire breakage. Prompt intraoperative decision-making, preparedness for retrieval techniques, and open communication post-surgery are key to mitigating adverse outcomes.
References
1. Parker MJ, Handoll HH. Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures. Cochrane Database Syst Rev. 2008;(3):CD000093.
2. Kuzyk PR, Bohl DG, McGee H, Schemitsch EH. Surgical management of intertrochanteric hip fractures: a comparison of fixed angle devices. J Orthop Trauma. 2009;23(6):465–470.
3. Gruber G, Giessauf C, Glehr M, et al. Failure of guide wires in hip fracture surgery: a retrospective analysis of 5,000 cases. Injury. 2008;39(8):796-800.
4. Streubel PN, Wong AH, Ricci WM, Gardner MJ. Implant removal after orthopaedic trauma: indications and outcomes. J Am Acad Orthop Surg. 2011;19(10):591–598.
5. Giannoudis PV, Tzioupis C, Pountos I, Papakostidis C. Surgical techniques: how to remove a broken guide wire from the femoral neck. Injury. 2007;38(12):1379–1383.
6. Mehlhoff TL, Noble PC, Bennett JB, Tullos HS. Metallic foreign body migration within the pelvis: a report of three cases. J Bone Joint Surg Am. 1982;64(4):599–601.
7. Choudhry MN, Abdallah A, Rashid RH, et al. Surgical errors and complications: a narrative review. Surg Technol Int. 2018;33:167-175.
| How to Cite this article: Kale S, Vatkar A, Srivastava S, Bhati A, Vyas A, Shyam A | Intraoperative Guide Wire Breakage during Intertrochanteric Fracture Fixation: A Technical Complication and Management Strategy | Journal of Orthopaedic Complications | May-August 2025;2(2):08-10. |